Understanding Chronic Kidney Disease (CKD)
- Dr. Ritu R. Vyas, MD

- Jul 14, 2025
- 12 min read
Introduction: Why Your Kidneys Matter More Than You Think
As a nephrologist — a physician who specializes in kidney disease — I have spent my career helping patients understand, manage, and slow the progression of kidney disease. One of the most important messages I share with every patient is this: chronic kidney disease often has no symptoms until it is already quite advanced. That is why education, early detection, and proactive management are not just helpful — they are life-changing.
This guide is designed to give you a thorough, honest, and medically accurate understanding of chronic kidney disease (CKD): what it is, how it is diagnosed, who is at risk, what you can do about it, and when to seek specialized care. Whether you have been recently diagnosed, have risk factors like diabetes or high blood pressure, or simply want to protect your long-term health, this resource is for you.

What Do the Kidneys Actually Do?
Your kidneys are two bean-shaped organs, each roughly the size of a fist, located on either side of your spine just below your rib cage. Despite their small size, they perform an extraordinary number of vital functions:
Filter approximately 200 liters of blood every single day, removing waste products and excess fluid as urine
Regulate blood pressure through the renin-angiotensin-aldosterone system (RAAS)
Balance electrolytes such as sodium, potassium, calcium, and phosphorus
Produce erythropoietin (EPO), the hormone that signals your bone marrow to make red blood cells
Activate vitamin D, which is essential for strong bones and immune function
Maintain acid-base balance to keep your body's pH in a healthy range
Clear medications, toxins, and metabolic byproducts from your system
When the kidneys lose function — even gradually — every one of these processes is affected. This is why CKD is not just a kidney problem; it has widespread effects on cardiovascular health, bone density, energy levels, brain function, and overall quality of life.
What Is Chronic Kidney Disease (CKD)?
Chronic kidney disease is defined as abnormalities of kidney structure or function, present for more than three months, with implications for health. The key word is chronic — meaning long-lasting and persistent, not temporary or reversible.
CKD affects an estimated 37 million adults in the United States — about 1 in 7 adults — yet the vast majority do not know they have it. Globally, CKD affects over 800 million people and is among the fastest-growing causes of death worldwide.
CKD is diagnosed when one or both of the following markers are present for at least three months:
An estimated glomerular filtration rate (eGFR) below 60 mL/min/1.73m²
Evidence of kidney damage, such as protein in the urine (proteinuria/albuminuria), structural abnormalities on imaging, or pathological changes on biopsy
The Stages of CKD: Understanding How Kidney Function Is Classified
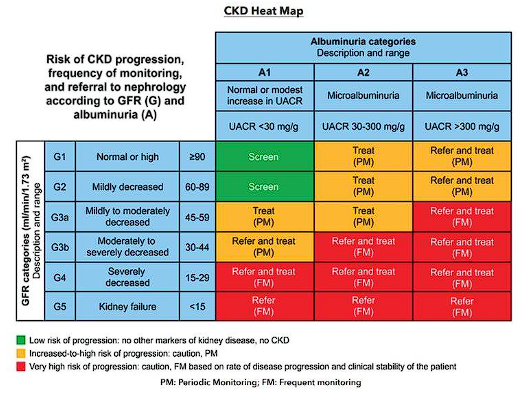
CKD is classified into five stages (G1–G5) based primarily on eGFR, and further categorized by the degree of albuminuria (protein in the urine). Understanding your stage helps your care team tailor treatment to your specific needs.
eGFR (mL/min/1.73m²) | Description | What This Means for You | |
G1 | ≥ 90 | Normal or High | Kidney damage present but function is normal. Identify and treat the cause; monitor closely. |
G2 | 60–89 | Mildly Decreased | Slightly reduced function, usually no symptoms. Lifestyle changes and BP control are key. |
G3a | 45–59 | Mildly to Moderately Decreased | Closer monitoring needed. Watch for anemia and early bone mineral changes. |
G3b | 30–44 | Moderately to Severely Decreased | Higher cardiovascular risk. Nephrology referral strongly recommended. |
G4 | 15–29 | Severely Decreased | Begin planning for kidney replacement therapy. Discuss dialysis and transplant options. |
G5 | < 15 | Kidney Failure (ESKD) | Dialysis or kidney transplant is required for survival. |
Important: Stage alone does not tell the whole story. Two patients at the same eGFR may have very different prognoses depending on the amount of protein in their urine, their underlying cause of CKD, and their other medical conditions. This is why individualized care with a nephrologist matters.
What Causes CKD? Common and Less Common Causes
The Most Common Causes
Diabetic Kidney Disease (Diabetic Nephropathy): Diabetes is the single leading cause of CKD and end-stage kidney disease (ESKD) in the United States, responsible for approximately 38% of new dialysis cases. Chronically elevated blood sugar damages the delicate filtering units of the kidney (glomeruli). Early diabetic kidney disease is often silent — detectable only by urine protein testing — which is why annual screening is essential for all patients with diabetes.
Hypertensive Nephrosclerosis: High blood pressure is the second most common cause of CKD. Over time, uncontrolled hypertension causes the small blood vessels within the kidney to thicken and stiffen, reducing blood flow and filtration capacity. The relationship is bidirectional — CKD also worsens hypertension, creating a damaging cycle.
IgA Nephropathy (Berger's Disease): The most common primary glomerular disease worldwide, IgA nephropathy occurs when IgA antibodies accumulate in the kidney's filtering units, triggering inflammation. Recent years have brought exciting new targeted treatments, making early diagnosis increasingly important.
Autoimmune Diseases: Conditions such as lupus (systemic lupus erythematosus), ANCA-associated vasculitis, and anti-GBM disease can attack the kidneys directly, causing rapidly progressive damage if not identified and treated promptly.
Polycystic Kidney Disease (PKD): A genetic condition in which fluid-filled cysts develop in both kidneys, gradually enlarging them and reducing functional tissue. Autosomal dominant PKD (ADPKD) is the most common inherited kidney disease, affecting approximately 1 in 400 to 1 in 1,000 people.
Other Important Causes
Recurrent or chronic kidney infections (pyelonephritis)
Kidney stones causing obstruction
Focal segmental glomerulosclerosis (FSGS) and membranous nephropathy
Alport syndrome (hereditary nephritis)
Medication-related nephrotoxicity (NSAIDs, certain antibiotics, contrast dye)
Obstructive uropathy (enlarged prostate, structural abnormalities)
Who Is at Risk for CKD?
Knowing your risk factors empowers you to take action before kidney function declines.
Risk Category | Examples |
Medical Conditions | Diabetes, high blood pressure, heart disease, obesity, recurrent kidney infections, kidney stones, lupus, vasculitis, IgA nephropathy, polycystic kidney disease |
Demographics | Age 60 or older; African American, Hispanic, Native American, or Asian American heritage |
Family History | First-degree relatives with kidney disease, dialysis, or kidney transplant |
Medications & Exposures | Long-term NSAIDs (ibuprofen, naproxen), certain antibiotics, IV contrast dye, nephrotoxic herbal supplements |
Lifestyle Factors | Smoking, chronic dehydration, high-sodium or high-protein diets, obesity |
Are You at Risk? These Two Tests Can Tell You. |
If any of the above apply to you, ask your healthcare provider for:
|
Signs and Symptoms: Why CKD Is Called the "Silent Disease"
One of the greatest challenges in CKD care is its silence. The kidneys have tremendous reserve capacity — you can lose up to 60–70% of kidney function before experiencing noticeable symptoms. This is why so many patients are surprised to learn they have significant kidney disease.
Early Stages (G1–G3): Often No Symptoms
In early to moderate CKD, most people feel entirely normal. CKD is often discovered incidentally during routine blood or urine testing. Occasionally, patients may notice:
Foamy or bubbly urine (suggesting protein loss)
Blood in the urine (hematuria) — sometimes only visible under a microscope
Slightly elevated blood pressure
Later Stages (G4–G5): Uremic Symptoms Emerge
As kidney function declines further, waste product buildup (uremia) causes symptoms that can profoundly affect quality of life:
Fatigue and weakness — often due to anemia from reduced erythropoietin production
Swelling (edema) in the feet, ankles, legs, or around the eyes from fluid retention
Shortness of breath from fluid in the lungs or anemia
Poor appetite, nausea, vomiting from uremic toxin buildup
Difficulty concentrating or mental fogginess ("uremic encephalopathy")
Muscle cramps, particularly at night, from electrolyte imbalances
Dry, itchy skin (uremic pruritus)
Decreased urination or changes in urine output
Bone pain or fractures from disordered mineral metabolism
Metallic taste in the mouth or ammonia-like breath
If you are experiencing any of these symptoms — particularly with known risk factors — please seek medical evaluation promptly.
How Is CKD Diagnosed? The Tests You Need to Know
Estimated Glomerular Filtration Rate (eGFR)
The eGFR is the cornerstone of CKD diagnosis and staging. It estimates how much blood your kidneys filter per minute. It is calculated from your serum creatinine, age, and sex. A single low eGFR is not sufficient for diagnosis — abnormalities must persist for at least 3 months to confirm CKD (ruling out acute kidney injury).
Normal eGFR: Generally 60 or above for most adults, though it naturally declines slightly with aging — the average person loses about 1 mL/min per year after age 40.
Urine Albumin-to-Creatinine Ratio (uACR)
Albumin is a protein that healthy kidneys prevent from leaking into urine. When filters are damaged, albumin leaks out — called albuminuria or proteinuria. The uACR quantifies this leak. Even with a normal eGFR, significant albuminuria is diagnostic of CKD and is one of the strongest predictors of progression and cardiovascular risk.
Albuminuria Categories |
A1 (Normal to mildly increased): uACR < 30 mg/g A2 (Moderately increased): uACR 30–300 mg/g A3 (Severely increased): uACR > 300 mg/g |
3. Additional Diagnostic Tests
Depending on clinical context, your nephrologist may order:
Complete metabolic panel — sodium, potassium, bicarbonate, phosphorus, calcium, BUN, creatinine
Complete blood count (CBC) — to assess for anemia
PTH and vitamin D levels — for bone health assessment
Renal ultrasound — to evaluate kidney size, structure, and rule out obstruction
Autoimmune workup — ANA, ANCA, complement levels, anti-GBM antibodies if glomerulonephritis is suspected
Kidney biopsy — when the cause is unclear or a treatable diagnosis needs confirmation
Complications of CKD: What Happens When Kidneys Fail Gradually
Cardiovascular Disease
Cardiovascular disease is the leading cause of death in CKD patients — more patients die from heart disease than progress to dialysis. CKD accelerates atherosclerosis, causes left ventricular hypertrophy, promotes inflammation, and disrupts fluid and electrolyte balance. Every reduction in eGFR category is associated with increasing cardiovascular risk.
Anemia of CKD
Reduced erythropoietin production leads to anemia, causing fatigue, reduced exercise tolerance, impaired cognition, and worsening cardiac strain. Management includes iron supplementation and erythropoiesis-stimulating agents (ESAs).
CKD-Mineral and Bone Disorder (CKD-MBD)
As eGFR declines, phosphorus accumulates, active vitamin D production falls, and PTH rises — secondary hyperparathyroidism. Left untreated, CKD-MBD causes weakened bones, vascular calcifications, and increased fracture risk.
Metabolic Acidosis
Failing kidneys cannot adequately excrete acid, leading to low blood bicarbonate (metabolic acidosis). This accelerates muscle wasting, worsens bone disease, and independently promotes CKD progression. Oral sodium bicarbonate is an effective, inexpensive treatment.
Hyperkalemia
As CKD progresses, elevated blood potassium (hyperkalemia) becomes a significant risk — it can cause dangerous heart arrhythmias. Management includes dietary potassium restriction and newer potassium binders such as patiromer and sodium zirconium cyclosilicate.
Fluid Overload and Hypertension
Impaired sodium and water excretion leads to fluid retention, worsening hypertension and potentially causing heart failure. Diuretics and strict sodium restriction are central to management.
How Is CKD Managed? A Comprehensive Approach
Blood Pressure Control
Target blood pressure in CKD is generally below 120–130/80 mmHg, particularly with significant proteinuria. Cornerstone medications include:
ACE inhibitors (e.g., lisinopril, ramipril) — reduce intraglomerular pressure and proteinuria
ARBs (e.g., losartan, irbesartan) — equivalent to ACE inhibitors, often better tolerated
These agents protect kidney function independently of their blood pressure-lowering effect
Blood Sugar Control in Diabetic CKD
Tight glycemic control slows diabetic kidney disease progression. Beyond traditional medications, newer drug classes have shown remarkable kidney-protective effects:
SGLT2 inhibitors (empagliflozin, dapagliflozin, canagliflozin) — now indicated for CKD even in patients without diabetes; reduce kidney disease progression, hospitalization for heart failure, and cardiovascular death
GLP-1 receptor agonists (semaglutide, liraglutide) — reduce albuminuria and support weight loss
Dietary Modifications
Nutrition is a powerful tool in CKD management. Key principles include:
Sodium restriction (2,000 mg/day or less) — reduces blood pressure and fluid retention
Protein moderation (0.6–0.8 g/kg/day for non-dialysis CKD) — reduces uremic waste
Potassium management — individualized based on lab values; NOT all CKD patients need restriction
Phosphorus limitation — avoid processed foods high in phosphate additives
Plant-forward diet — emerging evidence supports plant-based proteins and Mediterranean or DASH dietary patterns in CKD
Important: Dietary needs in CKD are highly individualized and change with disease stage. Please consult a registered dietitian with CKD expertise rather than following generic kidney diet advice online.
Avoiding Kidney-Toxic Exposures
NSAIDs (ibuprofen, naproxen) — reduce blood flow to the kidneys; use acetaminophen for pain instead, with guidance
IV contrast dye — notify your radiologist; pre-hydration protocols may be needed
Nephrotoxic antibiotics — aminoglycosides, vancomycin; always disclose your CKD to prescribers
Herbal supplements — many, including aristolochic acid-containing herbs and certain Chinese herbal remedies, are directly nephrotoxic
Managing Complications
Anemia: Iron studies, ESAs, and newer HIF-PHI agents (daprodustat)
CKD-MBD: Phosphate binders, active vitamin D analogs, calcimimetics
Metabolic acidosis: Oral sodium bicarbonate supplementation
Hyperkalemia: Dietary restriction, patiromer or sodium zirconium cyclosilicate
Fluid overload: Loop diuretics (furosemide), sodium and fluid restriction
Cardiovascular Risk Reduction
Statin therapy — most CKD patients benefit
SGLT2 inhibitors — dual kidney and heart protection
Finerenone (Kerendia) — non-steroidal MRA approved to reduce CKD progression and cardiovascular events in diabetic CKD
Preparing for Kidney Replacement Therapy (When Needed)
For patients approaching Stage 5, planning ahead makes an enormous difference in outcomes. Options include:
Hemodialysis — performed in a dialysis center or at home, typically 3 times per week
Peritoneal dialysis — uses the abdominal lining as a filter; performed at home, offering greater flexibility
Kidney transplantation — the preferred treatment for eligible patients; pre-emptive transplant before dialysis starts yields the best outcomes
I strongly advocate for early referral to a transplant center for appropriate patients, and for thorough, unhurried education about all options so patients can make choices aligned with their values and lifestyle.
When Should You See a Nephrologist?
Your primary care provider can manage early CKD, but there are specific circumstances where evaluation by a nephrologist (kidney specialist) is essential:
Indications for Nephrology Referral |
|
Exciting Advances in CKD Treatment: Hope on the Horizon
CKD care has been transformed over the past decade, and the pace of progress is accelerating. Here are the most important recent developments:
SGLT2 inhibitors: Dapagliflozin and empagliflozin are now FDA-approved for CKD regardless of diabetes status, with landmark trials showing 30–40% reductions in CKD progression
Finerenone (Kerendia): A novel non-steroidal mineralocorticoid receptor antagonist approved for diabetic CKD
Sparsentan (Filspari): A dual endothelin-angiotensin receptor antagonist; FDA-approved for IgA nephropathy to reduce proteinuria and slow progression
Tarpeyo (budesonide): A targeted-release oral corticosteroid FDA-approved for IgA nephropathy; delivers anti-inflammatory therapy directly to the gut-kidney axis
APRIL/BAFF inhibitors for IgA nephropathy: Iptacopan targets the complement pathway; sibeprenlimab (anti-APRIL) and zigakibart (anti-BAFF) are in late-stage trials with FDA Breakthrough Therapy designation — watch for approvals
Tavneos (avacopan): FDA-approved complement C5a receptor inhibitor for ANCA-associated vasculitis; replaces high-dose steroids in remission induction and reduces organ damage
HIF-PHI agents (daprodustat): Oral agents for anemia of CKD
Patiromer and sodium zirconium cyclosilicate: Novel potassium binders enabling patients to stay on RAAS-blocking medications
Implantable artificial kidneys: The Kidney Project at UCSF and other programs are developing bioartificial kidneys — early-stage but promising
If you have been told there is nothing more to do for your kidney disease, I encourage you to seek a second opinion. The landscape of treatment has changed dramatically.
CKD Risk Heat Map: Are You in a High-Risk Zone?
Taking Charge of Your Kidney Health: Patient Advocacy Tips
As a patient, you are the most important member of your healthcare team. Here is how to advocate for yourself:
Know your numbers: Ask for your eGFR and uACR at every relevant appointment and track trends over time
Bring a complete medication and supplement list to every visit
Do not skip nephrology follow-up appointments — CKD requires consistent monitoring
Ask questions: What is causing my CKD? What is my goal eGFR trend? Do I need a kidney biopsy?
Consider a renal dietitian consultation — dietary management in CKD is nuanced and personalized
Connect with support organizations: The American Kidney Fund and the National Kidney Foundation offer resources, financial assistance, and peer support
Plan ahead: If your CKD is advanced, start conversations about kidney replacement therapy early — ideally 12–18 months before you might need it
Address mental health: Depression and anxiety are common and underrecognized in CKD; ask for behavioral health referrals
The Bottom Line: Early Action Changes Everything
Key Takeaways for You and Your Family |
|
As a nephrologist, I believe that patients who understand their disease are empowered to fight it. The goal is not just to manage kidney disease, but to partner with you — giving you the knowledge, tools, and compassionate expert care to protect your kidneys for as long as possible.
If you have questions about your kidney health or would like to schedule an evaluation, please reach out.
References
This article is written for patient education and is based on current evidence-based guidelines and peer-reviewed literature. Key sources include:
Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2024;105(4S):S117–S314.
Centers for Disease Control and Prevention (CDC). Chronic Kidney Disease in the United States, 2023. Atlanta, GA: US Department of Health and Human Services, CDC; 2023.
Heerspink HJL, Stefansson BV, Correa-Rotter R, et al. Dapagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2020;383(15):1436–1446.
Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N Engl J Med. 2019;380(24):2295–2306.
Bakris GL, Agarwal R, Anker SD, et al. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes. N Engl J Med. 2020;383(23):2219–2229.
Kalantar-Zadeh K, Jafar TH, Nitsch D, Neuen BL, Perkovic V. Chronic kidney disease. Lancet. 2021;398(10302):786–802.
National Kidney Foundation. KDOQI Clinical Practice Guidelines for Chronic Kidney Disease. Am J Kidney Dis. 2002;39(2 Suppl 1):S1–S266. (Updated guidance at kidney.org)
Levey AS, Coresh J. Chronic kidney disease. Lancet. 2012;379(9811):165–180.
Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–1305.
Thurlow JS, Joshi M, Yan G, et al. Global Epidemiology of End-Stage Kidney Disease and Disparities in Kidney Replacement Therapy. Am J Nephrol. 2021;52(2):98–107.
United States Renal Data System. 2023 USRDS Annual Data Report. National Institutes of Health, NIDDK, Bethesda, MD, 2023.
Cheung AK, Chang TI, Cushman WC, et al. KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney Int. 2021;99(3S):S1–S87.
This article is for educational purposes only and does not constitute medical advice. Please consult with a qualified healthcare provider for personalized medical guidance.



Comments